Stage 3 Pressure Ulcer
Stage 3 pressure ulcers represent a serious wound with full thickness skin loss. The subcutaneous fat layer is now visible, indicating prolonged and severe tissue damage. These wounds require intensive treatment, take months to heal, and often indicate significant failures in nursing home or hospital care.
What Is a Stage 3 Pressure Ulcer?
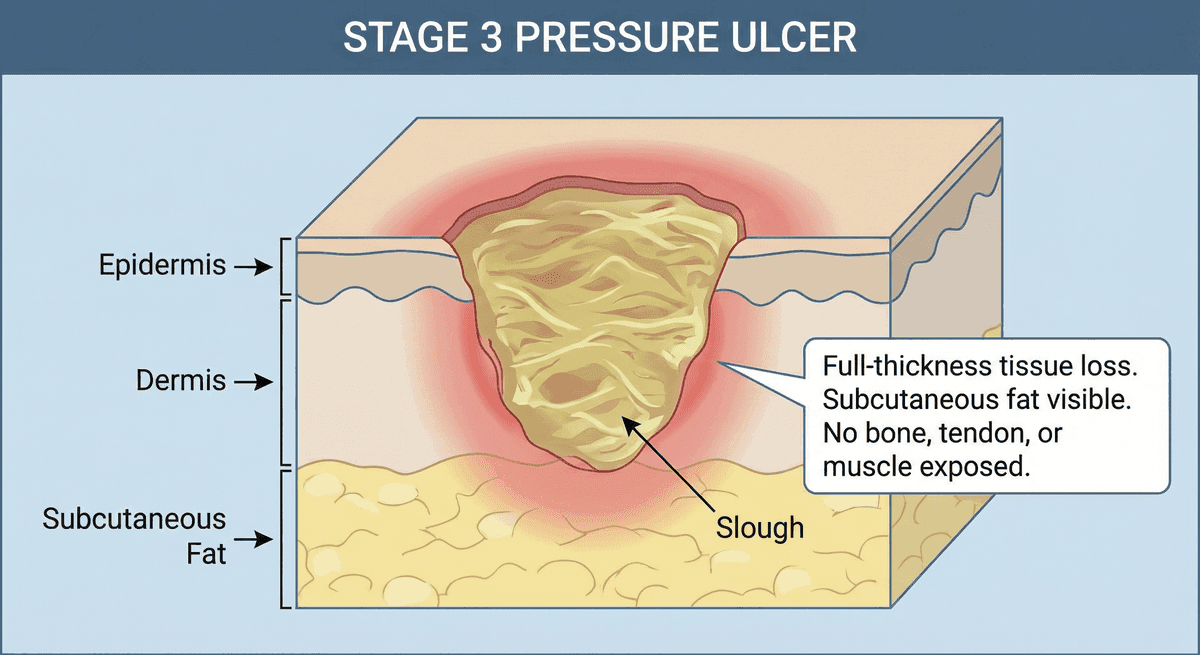
A Stage 3 pressure ulcer is defined by the National Pressure Injury Advisory Panel (NPIAP) as full thickness loss of skin. In Stage 3 wounds, the epidermis and dermis are both destroyed, and the subcutaneous fat tissue is visible in the wound bed. However, bone, tendon, ligament, and muscle are not exposed—exposure of those structures would indicate progression to Stage 4.
Slough (yellow, stringy, dead tissue) and eschar (dry, black, dead tissue) may be present in Stage 3 wounds. The depth of Stage 3 ulcers varies significantly depending on the anatomical location. In areas with thick fat layers (like the buttocks), the wound may be quite deep. In areas with minimal fat (like the bridge of the nose or ear), Stage 3 wounds may appear relatively shallow while still being full thickness.
The presence of slough or eschar does not change the stage classification. However, if slough or eschar obscures the wound bed to the extent that the true depth cannot be assessed, the wound may be classified as unstageable until debridement reveals the wound bed.
How Stage 3 Ulcers Appear
Recognizing Stage 3 pressure ulcers helps families understand the severity of their loved one's condition. Key visual characteristics include:
Wound Bed
- Fat tissue visible in the wound (appears yellow and lobular)
- Wound bed may be red, pink, or covered with slough
- Bone, tendon, and muscle are NOT visible
- Wound appears as a deep crater or cavity
Wound Edges and Margins
- Wound edges are distinct but may be rolled or thickened
- Undermining (tunneling under intact skin) may be present
- Surrounding skin may show signs of damage or previous injury
- Edges may appear macerated (white, soggy) if moisture is an issue
Dead Tissue (Slough and Eschar)
- Slough: Yellow, tan, or gray stringy tissue on the wound bed
- Eschar: Dry, black or brown, leathery dead tissue
- Mixed presentations with both slough and viable tissue are common
- Dead tissue must be removed for healing to occur
Why Stage 3 Is Serious
Stage 3 pressure ulcers represent a significant medical condition that carries substantial risks:
Extended Healing Time
Unlike Stage 1 or Stage 2 ulcers that may heal in days to weeks, Stage 3 wounds typically require months of treatment. Even with optimal care, healing is measured in weeks to months, not days. Some Stage 3 wounds require surgical intervention.
Infection Risk
Open wounds exposing fatty tissue provide an ideal environment for bacterial growth. The risk of wound infection increases dramatically with Stage 3 ulcers. Infections can lead to:
- Cellulitis (spreading skin infection)
- Abscess formation
- Osteomyelitis (bone infection)
- Sepsis (life-threatening blood infection)
Pain and Suffering
Stage 3 ulcers cause significant pain. The exposed tissue, frequent dressing changes, debridement procedures, and potential complications all contribute to patient suffering that could have been prevented with proper care.
Decreased Quality of Life
Patients with Stage 3 pressure ulcers face restrictions on mobility and positioning, prolonged hospitalization or specialized wound care, and reduced ability to participate in daily activities or therapy.
Why Stage 3 Often Indicates Negligence
Pressure ulcers do not suddenly appear at Stage 3. They progress through earlier stages, providing multiple opportunities for intervention. When a patient develops a Stage 3 pressure ulcer, it typically means:
Failure at Multiple Points of Care
- Prevention failure: High-risk patients should receive preventive care from admission. Standard protocols include risk assessment, specialty mattresses, and repositioning schedules.
- Detection failure: Regular skin assessments should identify Stage 1 changes before they progress.
- Treatment failure: Once identified, early-stage wounds require immediate intervention to prevent worsening.
- Monitoring failure: Wounds should improve with proper care, not deteriorate to deeper stages.
Timeline of Neglect
For a pressure ulcer to reach Stage 3, significant time has passed—often days to weeks of inadequate care. During this time, a facility had numerous opportunities to:
- Identify the patient as high-risk
- Implement prevention protocols
- Notice early skin changes during routine care
- Document and treat Stage 1 or Stage 2 wounds
- Escalate care when wounds did not improve
- Notify family members and physicians of deterioration
Each missed opportunity compounds the negligence. Stage 3 pressure ulcers represent systemic care failures, not isolated incidents.
Common Locations
Stage 3 pressure ulcers develop over bony prominences where pressure concentrates, similar to earlier stage wounds:
- Sacrum and coccyx (tailbone area): The most common location, accounting for a significant percentage of all pressure injuries. Deep wounds here can be particularly dangerous due to proximity to the spine.
- Ischial tuberosities (sit bones): Common in patients who spend extended time sitting in wheelchairs without proper pressure relief.
- Heels: The thin tissue over the heel bone makes this area vulnerable to rapid progression to Stage 3.
- Greater trochanters (hip bones): Common when patients are positioned on their sides for extended periods.
- Ankles and malleoli: Vulnerable when legs are not properly positioned or supported.
The depth of Stage 3 ulcers varies based on the amount of subcutaneous tissue at each location. Areas with more fat tissue will show deeper wounds.
Treatment of Stage 3 Pressure Ulcers
Stage 3 wounds require intensive, specialized wound care. Treatment protocols should include:
Debridement
Removal of dead tissue (slough and eschar) is essential for healing. Debridement methods include:
- Sharp debridement (surgical removal by a physician or wound care nurse)
- Enzymatic debridement (topical medications that dissolve dead tissue)
- Autolytic debridement (using body's own enzymes with moisture-retentive dressings)
- Mechanical debridement (wet-to-dry dressings, though less commonly used)
Advanced Wound Dressings
- Foam dressings for wounds with moderate to heavy drainage
- Hydrogels to maintain moisture in dry wound beds
- Alginate dressings for highly exudative wounds
- Negative pressure wound therapy (wound VAC) for some cases
- Antimicrobial dressings if infection is present or a concern
Pressure Elimination
- Specialty support surfaces (alternating pressure or low-air-loss mattresses)
- Complete offloading of the affected area
- Repositioning at least every two hours (more frequently if needed)
- Positioning devices to protect other at-risk areas
Nutritional Support
- High-protein diet (1.25 to 1.5 grams of protein per kilogram of body weight)
- Adequate caloric intake for wound healing
- Vitamin C and zinc supplementation may be indicated
- Hydration to support tissue perfusion
- Dietitian consultation for individualized planning
Surgical Options
Some Stage 3 pressure ulcers may require surgical intervention, particularly if:
- Conservative treatment fails to promote healing
- The wound is very large or deep
- Underlying bone infection (osteomyelitis) is present
- Tissue flap coverage is needed for wound closure
Complications of Stage 3 Ulcers
Without proper treatment or with continued neglect, Stage 3 pressure ulcers can lead to severe complications:
- Progression to Stage 4: Bone, muscle, or tendon exposure dramatically increases risks and treatment complexity.
- Wound infection: Bacterial colonization and infection delays healing and can spread.
- Osteomyelitis: Bone infection that may require surgical intervention and long-term antibiotics.
- Sepsis: Life-threatening systemic infection that can lead to organ failure and death.
- Chronic non-healing wounds: Some wounds become chronic and never fully heal.
Legal Implications
Stage 3 pressure ulcers carry significant legal implications for healthcare facilities. Federal regulations require nursing homes to ensure residents do not develop pressure ulcers unless clinically unavoidable, and that residents with existing wounds receive treatment to promote healing and prevent infection.
The presence of a Stage 3 pressure ulcer often indicates violations of:
- Federal nursing home regulations (42 CFR 483.25)
- State licensing requirements
- Facility policies and procedures
- Professional standards of nursing care
- The duty to provide adequate staffing
Documentation of Stage 3 wounds may trigger state surveys, deficiency citations, and in severe cases, criminal investigations. Learn about your legal options with a nursing home bedsore lawyer.
When to Seek Legal Help
If your loved one has developed a Stage 3 pressure ulcer while in a nursing home, hospital, or other care facility, you should consider consulting an attorney if:
- The wound developed while under the facility's care
- An earlier-stage wound progressed to Stage 3 despite treatment
- You were not promptly notified when the wound developed or worsened
- The facility has a history of pressure ulcer citations or deficiencies
- There appear to be staffing issues affecting care quality
- Your loved one has experienced complications from the wound
- The wound is not improving despite ongoing treatment
- You suspect the wound was understaged or concealed
At Traction Law Group, we help families understand what happened, obtain medical records and facility documentation, and pursue accountability when negligence has harmed their loved ones. A Stage 3 pressure ulcer represents preventable harm that facilities should be held responsible for. Find a bedsore lawyer or search our state directory to connect with representation in your area.
Documenting Stage 3 Pressure Ulcers
Thorough documentation is important for both ensuring proper care and preserving evidence for potential legal action:
- Photograph the wound with a timestamp if the facility permits—multiple photos showing size and depth are helpful.
- Request complete wound care records including measurements (length, width, depth), wound bed descriptions, treatment provided, and progress notes.
- Document the timeline—when you first noticed the wound, when you were informed by staff, and what stage it was at each point.
- Note treatments being provided—type of dressings, frequency of changes, use of specialty equipment.
- Keep records of all communications with facility staff about the wound and its treatment.
- Request the care plan to verify that the wound is addressed and appropriate interventions are documented.
This documentation can be invaluable in demonstrating the facility's knowledge of and response to the wound. For additional guidance, see our resource on how to document bedsores.
Frequently Asked Questions
- Q. What does a Stage 3 pressure ulcer look like?
- A Stage 3 pressure ulcer is a deep wound where the full thickness of skin has been lost, exposing the subcutaneous fat layer beneath. The wound appears as a deep crater and may contain yellow slough or black eschar (dead tissue). Bone, tendon, and muscle are not visible—if they are, the wound has progressed to Stage 4. The depth varies by body location.
- Q. Is a Stage 3 bedsore a sign of nursing home neglect?
- Stage 3 pressure ulcers strongly suggest inadequate care. These wounds do not develop suddenly—they progress through Stage 1 and Stage 2 first, providing multiple opportunities for intervention. According to CMS regulations, nursing homes must ensure residents do not develop avoidable pressure ulcers. A Stage 3 wound typically indicates failures in prevention, detection, and treatment over days to weeks.
- Q. How long does a Stage 3 bedsore take to heal?
- Stage 3 pressure ulcers typically require months of intensive treatment to heal, even with optimal care. Treatment includes debridement of dead tissue, advanced wound dressings, pressure elimination, and nutritional support. Some Stage 3 wounds may require surgical intervention such as tissue flap procedures. Without proper treatment, these wounds may never fully heal or may worsen to Stage 4.
- Q. Can you sue a nursing home for a Stage 3 bedsore?
- Yes. Families may pursue legal action when a Stage 3 pressure ulcer develops due to facility negligence. Federal regulations (42 CFR 483.25) require nursing homes to prevent avoidable pressure injuries and treat existing wounds. Traction Law Group helps families investigate how these wounds developed and works with co-counsel attorneys in your state to hold negligent facilities accountable. Consultations are free and confidential.
- Q. What are the complications of a Stage 3 pressure ulcer?
- Stage 3 pressure ulcers carry significant risks including wound infection, sepsis (life-threatening blood infection), osteomyelitis (bone infection), and progression to Stage 4. These wounds also cause chronic pain, require extended treatment, and reduce quality of life. According to medical literature, the mortality risk increases substantially once pressure injuries reach Stage 3 or beyond.
Sources & References
- Pressure Ulcer Stages Revised by NPUAP — National Pressure Injury Advisory Panel (NPIAP). Accessed January 2026.
- Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline — European Pressure Ulcer Advisory Panel, NPIAP, and Pan Pacific Pressure Injury Alliance. Accessed January 2026.
- Pressure Ulcers (Pressure Injuries) and Wound Care — Agency for Healthcare Research and Quality (AHRQ). Accessed January 2026.
- Long-Term Care Facilities: Guidance to Surveyors for Long-Term Care Facilities — Centers for Medicare & Medicaid Services (CMS). Accessed January 2026.
Your Loved One Has a Stage 3 Bedsore?
Stage 3 pressure ulcers rarely develop in facilities providing proper care. If your family member has a Stage 3 wound, contact us for a free consultation to understand what happened and explore your legal options.
Related Conditions & Topics
Stage 2 Pressure Ulcer
Partial thickness skin loss with exposed dermis.
Learn MoreStage 4 Pressure Ulcer
Full thickness tissue loss with exposed bone, tendon, or muscle.
Learn MoreBedsore Infection
Understanding infection risks in deep pressure ulcers.
Learn MoreSepsis from Bedsores
Life-threatening blood infection from untreated wounds.
Learn MoreGet Your Free Case Evaluation
Fill out the form below and our team will review your case immediately.